A digital health decade: driving innovation in Europe

Foreword
There cannot be a Digital Decade for Europe without health innovation. Digital technologies will be the key to unlock better health for all Europeans. Now the question is, will these innovations come from within Europe, or will we have to rely on the rest of the world?
Europe is home to a brilliant pool of health innovators already. DIGITALEUROPE’s 2020 and 2021 Future Unicorn Award winners were both AI-healthcare scale-ups. Yet, very often, health innovations start as ideas in Europe and then move to other markets, where soil is more fertile for them to grow and flourish.
Thus, we keep losing talent that could help us not only grow a fundamental sector, but most importantly, steer the development of new health technologies to ensure equal access to healthcare services and to safeguard universal health coverage.
This publication identifies promising health technologies on which Europe could take the lead, and offers a concrete policy roadmap to unlock their potential. Success depends on three key conditions: channelling investments, promoting health data flows, and enabling health technologies to be adopted at scale.
All this, however, will need to happen at multiple levels. First and foremost, at the EU level, where we see a myriad of overlapping regulatory proposals, such as the AI Act, the Data Act, and the European Health Data Space. In parallel, given that health is a primary competence of Member States, it is imperative that national and European policies are aligned and harmonised, especially when it comes to data protection, as well as data access and re-use for multiple purposes, from care to research. And finally, we must not lose sight of international collaboration, since health research is global – as the record development of COVID vaccines made clear.
This publication builds on our four pillars for a trusted and collaborative health data space. Trust and innovation are profoundly interdependent. Digital innovation in health is only impactful if it brings lasting benefits to everyone. As many of these innovations will inevitably mature in this decade, it will take decisive action from public and private leaders to make sure Europe is in the driving seat.



Why Europe should drive health’s digital transformation
There are several reasons why Europe is ideally placed to drive the digital transformation of health and care, but in order to fulfil this potential, there are some major challenges to overcome.
- Europe is home to some of the best healthcare systems in the world. These are generally closely intertwined with leading research institutes and companies, producing a treasure trove of health data. One example is Finland’s FinData, a first-of-its-kind national permit authority for the secondary use of health and social data. However, the EU still lacks a harmonised network for secondary use of health data at scale.
- Europe is building solutions to enable cross-border, privacy preserving and secure data flows. The General Data Protection Regulation (GDPR) created a global regulatory model for data protection and use while protecting fundamental rights. Its provisions need to be harmonised and clarified. The EU has also become a global leader in secure cross-border verification and validation of individual health data with its Digital Covid Certificate (over 700 million certificates issued to date). However, there is need to facilitate such secure systems for much more complex datasets.
- Europe’s approach to healthcare is already focused on delivering the best value for patients, and digital solutions can help address people’s needs equitably, ethically and securely, especially in underserved communities. For this to happen, however, regulations will have to be clear and harmonised. If we accelerate digitalisation, value-based care models – as opposed to fee-for-a-service – can be based on stronger evidence of improved patient outcomes.
- Europe’s research and development (R&D) is growing fast in sectors such as medical technology, pharmaceuticals, and biotechnology, but also in digital communication and computer technology. We have many potential unicorns at this intersection, such as Corti AI from Denmark (a member of IT-Branchen) and Oncompass from Hungary (a member of IVSZ).
Still, many health innovations start as ideas in Europe and then move to other markets where access to, and use of, reliable data at scale (e.g., for training AI) is easier. Despite all our strengths, the current fragmented landscape will not lead to innovations responding to the specific needs of a diverse population. We can and must reverse this trend to help everyone in Europe access ever more precise and personalised innovations.
In this paper, we identify three promising fields for Europe to lead in: connected health, precision medicine and digital twins. They are all solutions using digital technology enabled by data.
These fields of application are, among others, crucial for Europe to advance people-centred healthcare, tackling non-communicable diseases, beating cancer and addressing rare diseases. They will be also fundamental to strengthen our health systems, improving our response to and recovery from health crises.
People-centred healthcare everyone to make decisions and participate in their own care. It is organised around the health needs and expectations of people, rather than solely focusing on diseases.
This approach must underpin Europe’s health systems, especially as we look to encourage innovation and digital health technologies heavily relying on data. Trust from patients, healthcare professionals and society at large is a prerequisite for increased data flows. With a trustworthy Health Data Space, Europe can become the global hot spot and driving force for people-centred care, harnessing the opportunities granted by a Single Market for digital health solutions.
What digital solutions matter to people?
Patients are willing to use digital technologies for managing their health, provided these are developed with their needs at the core. That’s why patient experience should be a priority in eHealth and R&D. Digital solutions can strengthen the links between patients, healthcare professionals and innovators, both through applications being directly used by patients and practitioners, and technologies being developed for research purposes.
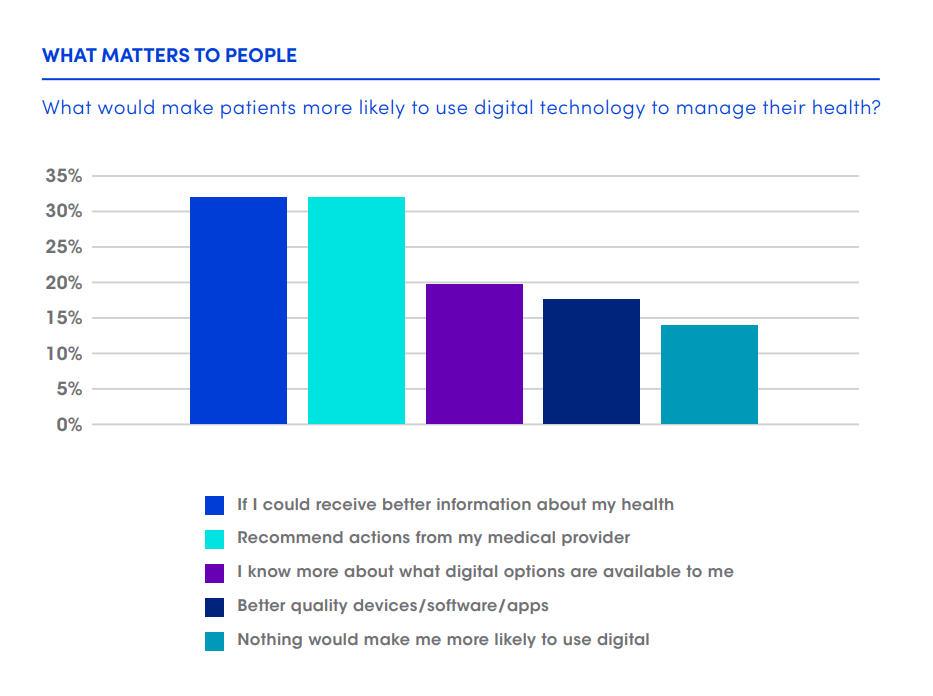
Source: Accenture
Measuring progress of the health data space project
In our 2019 manifesto for a stronger digital Europe, and later in our Digital investment plan for Europe’s recovery, we set out a list of success indicators to measure Europe’s digital progress. This same approach has been taken up by the European Commission in its Digital Decade strategy, and should be mirrored for digital healthcare and the EHDS.
of national and regional health budgets should be dedicated to digital health
should have secure access to their Electronic Health Records and they should be able to manage their own data including across borders. In 2021, these services are not a reality for most and the level of structured and standardised health data is low. We need concrete action to enable mutual recognition of:
-
Easy to use eID services. This service for identification and authentication is needed for enhanced cross-border access to health data and services for safer and continued care.[1]
-
A simple common consent form. In cases where aggregation and anonymisation of patient data is not feasible, and consent is the appropriate legal basis. The process is too complex now.
should have a single access point for secondary use of data. This will require:
-
All EU countries to have a central health data authority. These national entities should provide controlled data services, like healthcare information sharing and analyses. Where things stand, such permitting is fragmented, and centralised governance bodies only exist in 13 Member States.[2]
-
An EU-level entity for secondary use of health data: As a core tenet, the EU-level health data entity should promote the frictionless sharing of health data across Europe in a safe, controlled and privacy-preserving environment.
Ten ways technology can power Europe’s digital health decade
No continent alone can lead in all fields of health. We have identified ten key fields of application, in order of maturity, where Europe can drive innovation and have the greatest impact for patients, healthcare professionals, and ultimately society as a whole.
Attracting and retaining innovators and ensuring trust and uptake in these digital solutions can only happen through stronger collaboration between industry and government, among Member States, and through successful policy implementation at the national, EU, and international level. In Part 2, we outline a roadmap for legislators to achieve these goals.
Connected technologies for health services
Connected technologies for health help patients communicate with their providers no matter where they are (via telehealth and remote patient monitoring), and monitor their own health via apps, wearable and internal devices and other tools.
Connected health is more established in some areas than others, but especially in Europe there is room for growth. For example, 97% of biopharma executives in Europe say that growth opportunity for connected health exceeds that of more traditional businesses (as opposed to 78% in the US).
- Personalised care plans. Digital tools help people have a more central role in preventing diseases and managing their own health. Remote monitoring devices, for example, help collect more robust and longitudinal data, develop personalised interventions and tailored care plans (making patients more likely to comply with them), and facilitate follow-up by healthcare professionals.
- For instance, in cancer treatments, a digital ‘companion’ – a portal or application that complements medication with tools and information – can help both patients and practitioners take personalised clinical decisions, based on the patient’s clinical history, current status, and diagnostic reports. And it doesn’t stop here: molecular information could take personalisation to the next level.
- Preventative care. Shifting focus to prevention is the best way to invest in the population’s future wellbeing. For example, timely, personalised interventions made possible by predictive algorithms – fed by the data collected with remote monitoring devices – can help improve quality of life, by preventing chronic diseases and slowing down their progression. These insights can be combined with additional data, for example from the environment, to be even more accurate.
- For instance, medical devices can capture insights on heartrate, blood values (such as oxygen and glucose levels) or breathing patterns, monitoring trends and informing patients and care teams on preventative actions.
- Integrated care. When we think of complex health decisions, for example in chronic disease management, integrating different care services (from routine practitioner visits to advanced treatments, sometimes across different health systems) in a way that is smooth and accessible to patients must be a priority.
- For instance, digital platforms can now pair diabetic patients with nurses and care teams through connected sensors and devices, including in-app video chat and other call or messaging features.
- Digitalisation of surgery is using a range of connected health technologies including robotics and apps, helping patient care and experience before, during and after surgery by integrating data analytics to provide better insights to surgical teams. This helps medical interventions to be less invasive and more tailored, supports surgical training, and helps predict and reduce variability of patient outcomes.
- Remote consultation, monitoring and care. Remote care goes beyond pure ‘digitisation’ of care. For instance, it allows practitioners to prioritise in-person consultations for those at risk, while still delivering effective care to all their patients. It is also instrumental in addressing increasing health inequalities and ‘medical deserts’, i.e. those areas where fewer people have access to medical care. For instance, in France, 30 per cent of teleconsultations provided by Kry/Livi took place in a medical desert.
- The spread of remote care and telehealth has already proven beneficial for patients affected by cardiovascular and lung conditions. Over 60 per cent of European healthcare providers invested in telehealth initiatives in 2021, and plan to invest more in 2022.
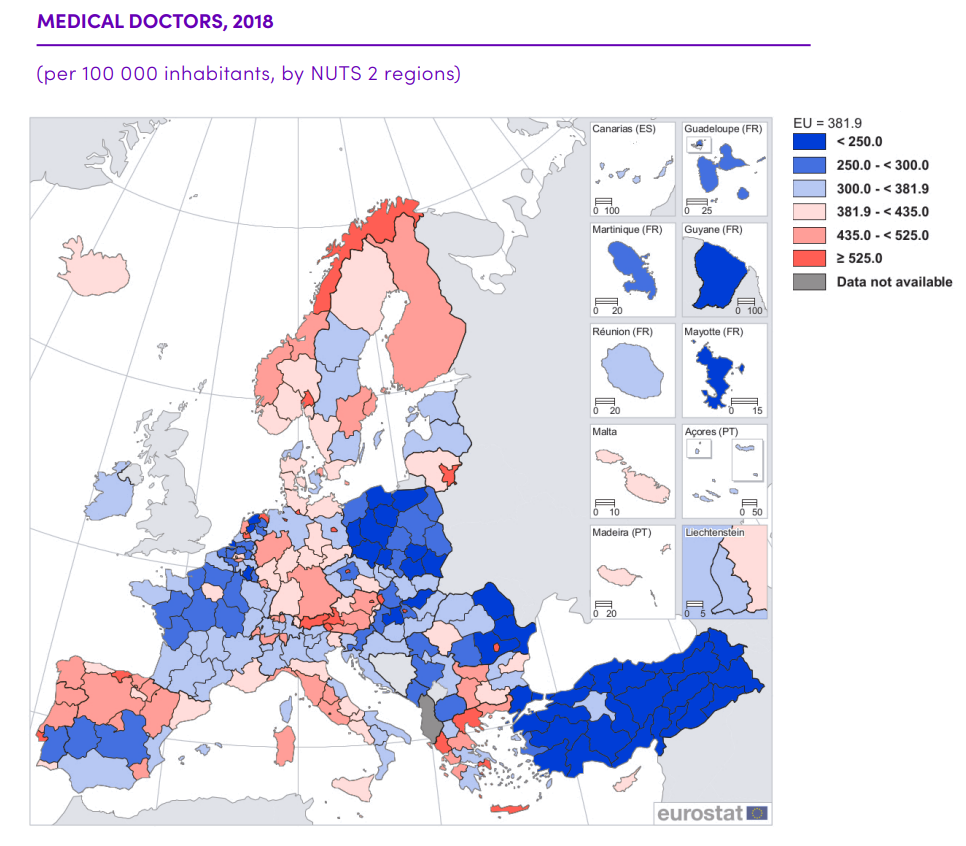
Source: Eurostat

“Large rural areas with a low population density and an ageing population are commonly those which experience medical deserts. Digital healthcare offers an important opportunity to address this challenge by providing primary care to patients from the comfort of their own homes.
For instance, in a rural region in northern Sweden, Kry/Livi collaborated with local authorities to address staff shortages and fragmented care in nursing homes. By using digital solutions for remote consultations, doctors from more densely populated areas were able to serve the rural areas of Västerbotten, improving both access to and continuity of care.
However, in numerous areas across Europe, patients are often limited in accessing remote consultations as regulations covering reimbursement have been formulated for physical care, without taking digital care into account.”
The availability of interoperable health data will underpin new and more effective population health management solutions. Advanced data analytics can be used to obtain insights based on several risk scores – such as medical history, demographic and socio-economic characteristics – and identify those groups who are most at risk, and would benefit the most from customised interventions. By incorporating socio-economic factors in their analysis, these technologies can improve access to quality care for underserved populations.
This is particularly relevant in the aftermath of COVID, as healthcare systems are struggling to reprioritise treatments and reduce waiting lists. Population health management solutions can identify at-risk patients, often with multiple conditions, who need to be treated without delay.
- Innovation and decentralisation of clinical trials and investigations. Clinical trials in Europe have traditionally been limited by the size of each country’s population, massively hindering scale and representation of patients, and delaying the development of life-saving treatments and medicines. Data science and digital technologies can help innovate clinical trials, minimising barriers to participation by using, for instance, wearables or telemedicine. This in turn increases diversity of data, including from the elderly and those living in remote areas.[3] Trials@Home provides an early example.
- Early indications show that decentralised clinical trials improve data quality by 41 per cent, recruitment of participants by 43 per cent, retention by 32 per cent, and time savings by 39 per cent. Companies are currently sponsoring 60 per cent of clinical trials in Europe.

“Dealing with different local legal requirements in the area of clinical trials – despite the overarching EU laws – makes it difficult for start-ups to enter new markets. For instance, ‘eConsent’ is not clearly defined at a European level. As a result, we have had to invest more internal time and resources to compensate for missing agreements on data privacy.”
Precision medicine
Precision medicine uses data such as molecular, genomic, and phenotypic information to provide insights and treatments that are tailored to individuals, rather than using a one-size-fits-all approach.
- Genomics. Analysing genomic data is a broad field that has a lot of potential to prevent diseases by better understanding a patient’s precise condition and hereditary background. However, it also relies on very large numbers of sequenced genomes.
- There are already steps in this direction. Europe’s 1+ Million Genomes Initiative aims to make this data accessible for research and innovation by 2022. However, we will need much larger numbers in order to make meaningful R&D advancements, ensuring accurate representation of the diversity of our population, and resulting in more effective innovations.
- Beyond that, linking genomic data with other health data (for instance, through the European Health Data Space) will create an even richer data pool to fuel the discovery and development of new treatments for patients. But the potential goes beyond R&D, for instance, for advanced diagnostic testing, where consistent access to genomic data will be key.

“A lot of medical practitioners in Europe are still rather sceptical about the adoption of new technologies in medicine. New technologies are usually implemented into clinical practice in the US first, and only later used in Europe. For example, multigene molecular profiling for precision oncology is now routine in the US, even being covered by Medicare, while in Europe it is mainly performed in large medical centres under research budgets.
This issue and Europe’s very fragmented market have slowed down the roll-out of the Realtime Oncology Treatment Calculator, our AI-based tool which supports oncologists to select the most appropriate molecular-based targeted treatment options for cancer patients.”
- Cell and gene therapies. Recent years have seen a steady acceleration in the number of cell and gene therapies on the market. But these therapies depend on supportive digital policies, as well as appropriate data infrastructure and governance, to enable real-world data and evidence.
- One promising technique in cancer treatment is CAR-T therapy, a type of treatment in which a patient’s immune system cells are changed in the laboratory so they will attack cancer cells.
- In children, three months after CAR-T infusion, 81 per cent of patients were in remission, as opposed to 20 per cent of patients treated with an alternative chemotherapy drug. In adults, patients were 2.5 times more likely to survive for two years post-treatment than patients treated with conventional treatment options.
Advanced models and digital twins
Digital models and twins can allow patients to access treatments and drugs that have been tested virtually instead of in real life, leading to a significant improvement in safety, efficacy, and speed in drug development, as well as reduced variability and increased surgery success rates.
- Tailored simulations of invasive procedures. Digital models of organs and other biological systems can help customise therapy or plan surgery. For example, companies in Europe have developed a digital twin of the human heart in order to tailor cardiological treatment to individual patients.[4] This involves simulation of invasive clinical procedures (such as stent insertion) in the digital heart which predicts outcome success in the real patient.
- Faster development of devices and medicines. Digital models and twins are also a tool to optimise therapies, increase safety as well as shortening the time to market for life-saving drugs.
- For instance, a simulation of drug delivery using digital twins of human lungs (for different models of patients with different particle sizes, inhalation rates, and initial locations) showed increased accuracy of 90 per cent, much higher than the 20 per cent common for conventional aerosol methods.
Synthetic control arms are digital models used for specific segments of population that cannot take part in clinical trials, such as some cancer patients. This is one of the major opportunities of digital twins, as it allows to augment or fully replace randomised controls.

Progress in digital health solutions is intrinsically linked to the developments in digital technology, notably AI and other data-intensive technologies. Companies develop new ways of delivering health using digital, but there needs to be a market for practical implementation to realise better outcomes for patients.
In Part 1, we outlined some of the digital health areas where Europe can take the lead. This, however, can only happen through stronger collaboration between government and industry, among Member States, and through successful policy implementation at the national, European, and international level.
The European Commission recognises that sustainable health technology innovation requires both pull (responding to existing demand) and push (actively creating, and taking up, new technologies) strategies.
Applying this to the EU’s health systems means steering the development of new health technologies to ensure equitable access to healthcare services and to safeguard universal health coverage through and for digital health. If we don’t actively pursue this goal, Europe’s role will be limited to pull factors, having to rely on innovations whenever, wherever and however they happen.
The European Health Data Space is a make-or-break moment for Europe to develop a Single Market for digital health and health data that is aligned to global developments, and that can also represent a successful model of data governance for other proposed Data Spaces.
Such a vision for Europe’s digital health decade means moving away from our current policy approach (ad-hoc response to challenges and crises) towards a long-term commitment to strengthen our health systems.
This will rely on the need for protected, sufficient and long-term investments; on robust and harmonised frameworks for health data flows; and on enabling health technologies to be adopted at scale.
Investing in the digital transformation of health systems
Europe needs an ambitious, long-term investment strategy in the digital transformation of health. We should keep in mind, however, that return on investment will only show after several years, so it’s important to earmark appropriate resources to bridge this period and support national and regional healthcare communities (including patients, healthcare professionals and health associations) while investment strategies are carefully coordinated and monitored.
There is much at stake. In the end, the potential for relocating resources to patient care and medical training are enormous. Across the OECD countries, uptake of data and digital technologies in health can, in a conservative estimation, result in a 30 per cent decrease in waste and inefficiencies (approximately €357 billion per year). With such savings, there are major opportunities for reinvestment in care, training and education.
At the European level
While Member States will ultimately have the responsibility over their respective health systems, the EU can support with investment and coordination.
- Coordinating digital transformation. The annual State of Health in the EU and the Digital Decade 2030 targets should be monitored together in order to produce tailored recommendations for Member States. The EU has a growing toolkit available to coordinate country-specific recommendations, such as the renewed European Semester, the annual cycles of the “State of Health” with the OECD and the Observatory on health systems, and the anticipated WHO Digital Health European Strategic Resource Kit.
- The anticipated WHO toolkit can provide a framework for assessing digital maturity levels of countries and regions, spanning from ‘establishing’, to ‘developing’, to ‘scaling up’ and finally ‘transitioning’. When linked to the European Semester framework and to the Digital Decade targets for skills, government, infrastructure and business, these can then inform budgetary recommendations.
- Freeing up EU funding to build the EHDS. Europe’s digital ambitions for health will need a bigger financial backing. This will have to come from both Member States and the EU, while leveraging private investment. The EU can allocate funding from several sources.
- The annual EU4Health budget dedicated to the set-up and operation of the EHDS must increase significantly from the 2022 one, which allocated between €80 and €100 million. We estimated that an increase of at least twice that amount would be required. Note that scaling up the EHDS will multiply the effectiveness of spending on other health-related pillars of the EU’s budget, such as resilience and beating cancer.
- More is needed. The EU budget for the period between 2021 and 2027 has earmarked a mere €5.3 billion for the EU4Health programme for a population of 447 million Europeans. This won’t be enough to unlock the innovations we need for the digital health decade.
- Facilitate efforts to boost digital health skills. At the current rate of investments, it is estimated that only 65 per cent of EU adults will have basic digital skills by 2030, far from the 80 per cent target in the Digital Compass. A way to reverse this outcome is an EU multi-country initiative on digital health education, financed through the Recovery and Resilience Facility.
- Other programmes should complement these efforts. The Commission’s Digital Education Plan should have a strong health focus in its advanced digital skills objectives. Regional authorities and the Commission should also develop inclusive projects targeting the digital health divide, to be financed through European Regional Development Funds and the European Social Fund.
- Harness private-public initiatives to boost research and development. The health sector is Europe’s strongest R&D performer, accounting for 20 per cent of the EU’s R&D investment. At the same time, more needs to be done to increase the attractiveness for research to stay in, or come to, Europe. For instance, in biotechnology, the R&D growth of US companies is remarkably higher; in 2020, R&D investment was 11 times larger than the EU, with 166 companies showing growth, compared to only 20 in Europe.
- Decreasing unnecessary legal burden and regulatory fragmentation, coupled with public investments, can help mobilise private capital and increase the role of private companies in growing European health excellence.
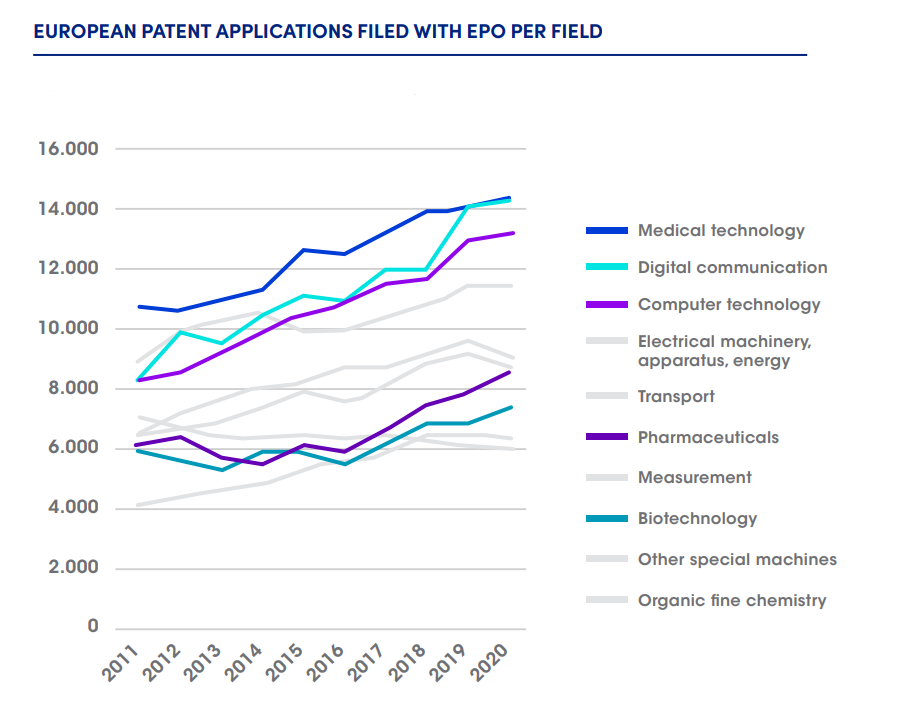
Sources: European Patent Office, European Commission
At the national and regional level
Member States and regions can coordinate investments and initiatives in line with the Digital Decade and EU health targets, including specific digital health targets as part of their national plans.
- National coordination of health-IT and digital health investment. While the earliest adopters of digital health, such as the Nordics, have championed a region-led approach, increasing calls for national centralisation can be heard. Major roadblocks are the lack of standardisation and the burden of legacy systems (highly relevant for addressing cyber vulnerability and resilience).
- Member States can learn from this experience and channel funding towards secure, federated and interoperable data infrastructure, which would facilitate the adoption of standards needed to scale up AI in clinical practice.
- Securing connected health devices. As use of 5G in healthcare increases, with applications in robotics, Internet of Things and AI, a new connected healthcare ecosystem will take shape. This raises the urgency for solid frameworks and investments by Member States and regions in connectivity and cybersecurity, as well in semiconductor production and supply to power these connected devices.
- In addition, we must not forget the urgent need to train cybersecurity specialists, as the EU lacks approximately 291,000 of them.
of medtech companies have chips in over half of their products.
- Support the digital transformation of healthcare organisations. Digital transformation not only improves clinical decision-making, but also helps healthcare organisations become more efficient and deliver better patient care. Concrete areas where digital technologies can support hospitals are care delivery, patients flow, organisation of staff, automation and supply-chain. This will require investments in better digital infrastructure and in modernising care facilities.
- Equip the healthcare workforce with digital skills. Not only do we need more doctors and nurses, but we need to train them for existing and future health-IT services and devices that will be vital to ease their work, for instance in automatising administrative procedures and freeing up time for patients. Digital skills for healthcare professionals should be ensured both through education curricula and continuous professional development.
Promoting health data flows through governance and standardisation
For Europe’s innovative health sector to thrive, it is imperative to have a solid governance framework for health data. This will provide greater clarity and certainty on the protection of people’s fundamental rights, while at the same time unlocking opportunities in digital health research and development.
The GDPR provides a framework in which such certainty could be built, yet shortcomings in its implementation have created an unnecessarily fragmented landscape for data protection.[5]
Some Member States are more advanced in their approach to facilitating access to data for research (for example, Finland’s FinData), while others have no such framework in place, reinforcing the need for more harmonisation across the EU.
Beyond the governance of health data, a strong framework is needed to converge towards an agreed set of industry-driven health data standards for mutual interpretability and interoperability.
At the European level
- Getting the European Health Data Space right. While the proposed EHDS is meant to address national fragmentation of health data governance, we should learn our lessons from the GDPR and ensure that its implementation will not result in the same, or even increased, fragmentation. Industry-driven initiatives are making progress, but regulation is needed to allow for reuse of health data at scale. Gaia-X and other industry-driven or public-private platforms[6] have made progress at a smaller scale to define and address any technical and governance hurdles.
- In addition, given the EHDS builds on the EU Data Strategy, we must be careful in not simply duplicating the same shortcomings: a truly harmonised EU data framework will only unleash the value of the data economy if regulation is flexible enough to foster future innovation, rather than imposing a set of restraining obligations.
- Harmonising national application of the GDPR. This framework for data protection remains vital for health data to be used for care or research. However, it will still require harmonisation of data protection rules across Member States, and approaches for anonymisation and de-identification methods through guidelines from the European Data Protection Board (EDPB).
- Ultimately, clarity on protection of personal data can only be achieved through guidance from the EDPB, which will be instrumental in clarifying layers of legal complexity for research, development and entrepreneurship emerging from increased data availability.
- Create a European Digital and Health Data Board based on dialogue and collaboration. When setting up a body tasked with implementing the EHDS, it will be vital that all stakeholders take part in its governance, from patient associations (as improving patient wellbeing is the main goal) to research and industry (which will be the ones reusing health data for innovation).
- Facilitate cross-border health data sharing. The European Commission can facilitate the secure use and reuse of health data, for both primary and secondary purpose, by:
- Coordinating the implementation of the EHDS in Member States;
- Promoting the use of industry-driven data standards;
- Allowing for flexible arrangements for data processing services.
- Complete alignment will be key as Member States also play a role, for example through collaboration on baseline principles for digital health, while many public and private sector standards are already in place too.
- We have recently had two very successful examples of European collaboration: the EU Digital Covid Certificate and MyHealth@EU. Now, it is time to extend these learnings to more complex datasets (both within and across borders) such as for research and AI development. These will require robust systems for verification but also efficient data operations, with the aim of balancing usefulness of information and security limitations.[7]
At the national and regional level
- Addressing fragmented data rules and infrastructure within Member States. A majority of citizens is willing to share their health data for purposes such as better quality of care and empowerment in their prevention, diagnosis and treatment, a figure that comes close to 100 per cent for patients with rare diseases.
- Integration of national health information systems is needed to meet people’s expectations for personalised care and allow them to share medical data in a secure and fair way.
At the international level
- Transatlantic cooperation on digital health. Patients on both sides of the Atlantic should have access to trustworthy, digitally-supported healthcare. To generate this trust, the EU-US Trade and Technology Council (TTC) should find an agreement on frameworks for clinical and real-world data analysis and evidence needed for safer and more effective diagnosis and treatment. We outline more detailed recommendations for the TTC in the annex.
- Alignment in global health data codes and standards. Health systems around the world use a mix of codes for diseases (for instance, ICD11, READ, WHO) and the way those codes are used can differ a lot. Adopting the agreed and globally aligned coding standards across the EU and harmonising their use is critical for meaningful use of health data.
- One way to speed this up is by using AI to register these different codes using speech or text recognition. Such tools can be used in a care setting or to efficiently compile large amounts of mutually interpretable datasets.[8]

“Practical needs for real-world use cases are often not a priority for those curating standards. For instance, the current code sets used for vaccines in the global standards for patient summaries lack the required precision for making clinical decisions from life-long vaccination history.
That’s why Syadem had to develop its own way to re-encode vaccination trails found in physical and digital vaccination cards. Within our study for a European citizen’s vaccination card, we proposed to make this terminology and its alignments with the pre-existing codes publicly available.
We must agree on terminologies that strike the right balance between the irregular, individual reality of real-life medicine, and the need for structure and consistency in standards.”
Enabling health technologies to be adopted at scale
Both larger and smaller companies have found it difficult to roll out new innovations in Europe. This is due to, on the one hand, fragmented market access requirements, data availability, standards, and reimbursement schemes, and on the other hand, to rigid systems and delayed recognition of new digital applications for prevention, diagnostics, treatment and care. For example, for advanced diagnostics, a 5-to-10-year delay from initial launch to patient access is not uncommon.
As products and services become more digital, horizontal regulations such as those for AI and data protection risk further slowing adoption in Europe. To prevent this, we must foster the generation and use of quality data, also from a non-clinical setting, while allowing for faster and less cumbersome adoption, increasing safety and reliability along the way.
At the European level
AI should be seen as neither a silver bullet nor as a mere buzzword. In fact, there are already at least 50 tangible examples of AI’s ability to help deliver better outcomes, such as faster detection of tumours, strokes and other conditions. The next great leaps for AI in a clinical and wellness setting can happen in Europe if ethical aspects, perceptions and regulations allow for this.
- Clear rules for AI health applications. Ethical aspects of AI are to some extent already addressed in the existing horizontal and sectoral legislation, such as the GDPR and the Medical Device Regulation (MDR). In addition, in recent years several AI ethics frameworks have appeared, and the Commission has proposed an AI Act with requirements for trustworthy AI to protect fundamental rights and European values.
- In the specific case of the MDR and the In-vitro Diagnostics Regulation (IVDR), there is a serious risk of misalignment and duplication. Because the proposed AI Act defines high-risk AI systems broadly, almost all medical device software may fall in its scope and be considered high risk, even though the MDR and IVDR already set extensive and detailed requirements (some going beyond what is proposed in the AI Act). Yet the proposed definitions and requirements are not aligned, or are missing (e.g. definition of ‘risk’).
- For some devices, the proposed requirements may conflict with safety and performance requirements of the MDR and IVDR. This would lead to legal uncertainty for industry and competent bodies. It would also induce higher complexity and implementation costs for all healthcare actors (including hospitals, healthcare professionals and patients) and negatively impact the proper implementation of the MDR and IVDR.
- Ensure data access and use for training and testing AI. To be reliable, AI applications will need a huge amount of data. Currently, almost 70 per cent of entities developing AI technologies obtained data through their own collections (for example via clinical trials) as it was easier and cheaper. Opening up real-world sources (such as hospital Electronic Health Record systems) will further add to that potential.
- Embrace the utility of Real-World Data (RWD). Evidence generated or enriched using RWD can accelerate roll-out of new treatments in a safer way. This can be used to inform treatment options as well as facilitating implementation of reimbursement models with strict evidence requirements (outcomes-based or conditional). To empower both large and small companies, administrative burden can be minimised by working with an existing registry, including those used for regulatory mandated studies.
- However, many regulatory bodies in Member States (such as medicines agencies) have neither the infrastructure nor the expertise in place to enable the validation and post market monitoring using RWD (data generated in a non-clinical setting).
- Still, Europe is making progress under DARWIN. Now is the time to recognise the quality and validity of this evidence throughout the EU. Industry driven initiatives such as the Innovative Medicines Initiative have greatly contributed to Europe’s progress in this field. It will be important to work towards a more open and collaborative network for RWD interrogation, including industry as a partner.
DIGITALEUROPE’s Executive Council for Health

In July 2021, DIGITALEUROPE launched its Executive Council for Health to bridge the gap between business and policy expertise, and to advance the digital transformation of the health industry. The Council – comprising 20 senior executives from leading health and technology companies – encompasses Future Unicorn Award winning small and medium-sized companies (SMEs) and leading firms with many decades of experience in digital health.
The Council members collaborate to provide unique insights to policymakers on how digital can address urgent healthcare challenges. Unequivocally, trust and the roadmap for the European Health Data Space (EHDS) are the first concern, as they are foundational to the EU’s ambitions.
We support the European Commission’s ambition to enable sharing of data for healthcare, create a genuine single market for digital health products and services, increase access to health data for research, innovation, and policymaking, and foster the use of artificial intelligence in health.
To this end, we are aware of our role. Industries can do much to support the integrated network of academia, SMEs and public-private partnerships in healthcare, and therefore we understand our responsibility in fostering trust and support for the EHDS. We invite representatives of patients, clinicians, healthcare providers, regulators, and other groups to engage with us.
Our recommendations for key health data policies
- Building trust with EU citizens on data sharing initiatives involves structurally demonstrating results on issues that are meaningful to people’s everyday health and life. It needs to be possible for anyone in Europe to see real world outcomes of care and treatment, whilst supporting research for innovations in healthcare.
- The EHDS should align with current and developing legal frameworks. Read our positions on:
-
- How to make the most of the GDPR for research: There is still too much uncertainty across the EU around how health research can be conducted in accordance with data protection rules, and Guidelines from the European Data Protection Board should aim to remove as much of this uncertainty as possible. Resolving these issues is necessary to make the future EHDS possible and successful. Codes of Conduct for health research could be helpful.
- The Data Governance Act: The EHDS is an opportunity to make the benefits of this new legislation tangible in a sectorial setting. The Act lays out the foundational provisions for data sharing within the European Data Spaces, and also addresses the re-use of sensitive data held by the public sector, including in healthcare. The governing bodies in both this Act and the EHDS should include the stakeholders in scope, for the latter including at least patients and industry.
- The AI Act:The AI Act: Ensuring consistency and synergies with the existing EU regulatory framework is key (from GDPR to MDR). The EHDS should enable trustworthy AI by facilitating access to representative and fit for purpose data.
- The Data Act : This legislative proposal sets the right ambitions of boosting data sharing in Europe. However, some of the data access and sharing provisions will require further clarification and should strive to enable the re-use of data without setting excessive and restraining obligations. Regarding specifically governments’ access to companies’ data, creating an EU-wide framework is a good step to avoid regulatory fragmentation but access rules should be strictly defined, harmonised and not open to abuse. Finally, as data flows are vital to Europe’s economy, the Act should avoid restricting international data transfers beyond the provisions set in the GDPR.
- In our response to the consultation on the EHDS we called for the coordinated promotion of system-wide interoperability for both primary and secondary use of data. This should build on a system of incentivisation to boost mainstream health systems’ adoption of Europe-wide interoperability standards. For further processing of health data, we should co-create ethically acceptable incentives, governance models and establish multi-country data sharing collaborations.
- Clarify and harmonise conditions for the secondary use of health data.
- Member States should cooperate more in using interoperable standards and eID, delivering faster on initiatives.
- The EHDS framework should include mechanisms for broad participation and data use, including through altruism schemes, for both bigger and smaller companies. Scientific research is not only conducted by academia or public research institutes but also by private sector-stakeholders who, by developing innovative products and services, are an integral part of the healthcare ecosystem.
- The EHDS framework should safeguard European industry’s competitiveness in the international field.
Our health recommendations for the EU-US Trade & Technology Council
This is where the EU-US Trade & Technology Council can make a difference for innovative health companies and patients:
For the next TTC meeting
- Establish a joint task force for health data to:
- Discuss and collaborate on common data interoperability standards and exchange formats for health data (on SAAMD, genome profiling, biomarkers) to improve data use and re-use potential.
- Develop a coherent approach to access and processing of data to help address preparedness for pandemics, and rare and chronic diseases.
- Draw up a set of contractual clauses for transatlantic health data transfers.
- Agree on common definitions for pharmaceutical research and regulatory purposes, such as for Real World Data and Evidence. Generally, even on the conceptual level divergence exist between the EMA and the FDA.
In one year
- Work towards a mutual recognition agreement between the FDA and EMA to harmonise recognition of evidence data of in-silico trials for Advanced Therapeutic Medical Products (ATMP).
- Establish a working group with representatives from industry, EDPB, Commission and FTC to compile information on experiences with health data transfers and how issues can be addressed.
- Develop a template data use agreement and consent form clause that will facilitate data transfers, and which can be adopted by EU-US researchers, pharmaceutical and medical device companies, and healthcare providers.

“AI has the power to improve healthcare outcomes, for which it needs data. It will be key to aggregate data sets from the US and EU to build representative and effective solutions, therefore we need a sustainable and clear agreement for transatlantic data transfers.”
References
[1] Recital 10 of the eIDAS regulation (No 910/2014) refers to the requirement for the eHealth Network based on the cross-border healthcare to produce guidelines on cross-border access to electronic health data and services, including by supporting ‘common identification and authentication measures to facilitate transferability of data in cross-border healthcare’.
[2] This is reported on page 98 of the European Commission’s Assessment of the EU Member States’ rules on health data in the light of GDPR. Member States use divergent governance models.
[3] This field is moving fast and in the US the FDA has already issued its Guidance for Digital Health Technologies for Remote Data Acquisition in Clinical Investigations (2022).
[4] See for instance Siemens Healthineers’ example of a digital twin of the heart; GSK’s 3D models of tumour cells; and Dassault Systèmes’ virtual twins of humans.
[5] There is a growing and converging body of literature that collects evidence for the need of improvements to health data flows, such as from TEHDAS, the Assessment of the EU Member States’ rules on health data in the light of GDPR, Cross-border interoperability of Electronic Health Records, and the Study on eHealth, Interoperability of Health Data and Artificial Intelligence for Health and Care in the European Union.
[6] Gaia-X, association for data and cloud AISBL, the Global Pathogen Analysis System (GPAS) , the Augmenting Therapeutic Effectiveness through Novel Analytics (ATHENA), EuCanImage, and many more.
[7] For instance, Public Key Infrastructure, sometimes blockchain technology, can be used for smart contracts, aiming to achieve security without excessive loss of efficiency in data processing. More information can be found in the EU Blockchain Observatory and Forum’s (2022) Blockchain applications in the healthcare sector. (pp. 8, 17).
[8] See for instance Optum’s Impact Pro advanced data analytics tool which helps identify individuals who would benefit from tailored intervention programs based on ca. 1800 clinical markers. To localise this tool to the UK required mapping almost 600,000 codes.
